Advocates for clients who have been neglected or underrepresented in the system
During my third fieldwork rotation, I worked with individuals who were diagnosed with mental illness. Prior to arriving to the facility, many of them may have experienced trauma (physical, emotional, sexual, psychological), grown up in foster care, or lived on the streets. Many of these individuals have expressed that they honestly believe "no one loves them" and the odds of finding "someone who will ever love them enough to provide support and advocate for them," especially through a crisis, seems "impossible". Over time, these individuals have come to believe this because so many people in their lives have repeatedly never supported them (emotionally, socially, psychologically, spiritually, etc.), that they lose hope in others as well as themselves. They start to believe that they can't make it on their own because they haven't been able to do it so far. In turn, these individuals become reliant on others, who may not be helpful to the individual's quality of life and overall success, and develop poor or even toxic habits. Poor habits may include increased alcohol consumption or drug use; and toxic habits may include prostitution or getting involved in an abusive relationship. These habits can become barriers to an individual's reintegration into the community. For instance, these habits may exacerbate symptoms of a diagnosis, such as hallucinations, delusional verbalization, self-harm, suicidal ideation or suicidal attempts. When symptoms are intensified it can lead to hospitalization if the individual becomes dangerous to self. At the hospital, these individuals receive psychotropic medications until they are stable and no longer considered a threat to themselves. They are then released back into the community. However, these individuals don't receive the support and skills from the hospital upon release. This sets them up for failure because they don't have the basic skills necessary to function and reduce the likelihood for relapse post-discharge. This is when these individuals face obstacles while reintegrating into the community.
I had the pleasure of working with a 19-year old girl who was admitted to our facility due to a lack of social skills. Prior to doing the OCAIRS on her, I wanted to establish rapport so we chatted for a little while and I learned that she wasn't really aware of her diagnosis. As I interviewed her using the Occupational Circumstances Assessment Interview and Rating Scale (OCAIRS), I learned that she was diagnosed with schizoaffective disorder. She still didn't know what it meant and my fieldwork educator explained it to her. I also learned that she had an IEP throughout school and graduated within the last 12 months with her high school diploma. Her situation became more complex: not only did she have schizoaffective disorder -- which already presents with difficulty understanding verbal and non-verbal cues -- but she had an intellectual disability coupled with it.
Based on her interview, I was able to gather that my client did not receive as much help in developing basic social skills needed to successfully transition into the community post-graduation. This may have been due to cultural and environmental influences. Nevertheless the stigma of her intellectual disability limited her ability to participate in certain activities at home, at school, and in the community. She was continuously restricted to certain tasks over her lifetime she felt incompetent to try something new. For instance, she would stick to tasks she knew how to do because she had always done it at home or school. The same held true for new social experiences: she was uncomfortable interacting with anyone outside of her family. This resulted in her lack of desire to try new things and led her to believe she would never be able to live without a caregiver. Due to this lack of experience, it may have resulted in poor social skills. I learned that individuals with schizoaffective disorder not only have difficulty expressing themselves through facial expressions, tone, and body language, but they also have difficulty reading these nonverbal cues in others. Her dual diagnosis may have made it even more difficult to appropriately interact with others and led to social problems while in the community. This was one of the major reasons for my client to attend this program because she needed to improve her social interaction skills.
Towards the end of this interview, I learned that this young lady was a motivated individual who wanted to improve her social skills in order to eventually hold a job for more than a few months. Regardless of her intellectual disability and her mental illness, her motivation would be the catalyst to her overall success when working toward her social skills goal. Although I have worked with individuals with intellectual disabilities since high school, and I have seen numerous times that they are capable of learning something new, even at a slower pace, I had never worked with an individual with a dual diagnosis like this. The same was true for some of my other coworkers who had acknowledged to me that they were less familiar with individuals with intellectual disabilities, and more so with a dual diagnosis. I considered this to be an educational opportunity for both me and my coworker, but I also considered this to be a chance for me to advocate for this particular individual.
I started advocating for this individual to other staff members at my facility.
Luckily, they understood what I was saying, and gave me free reign to work with her. She was motivated to get started. Although she required frequent one-on-one sessions and repetition, her efforts began to show as she started making progress in her goals.
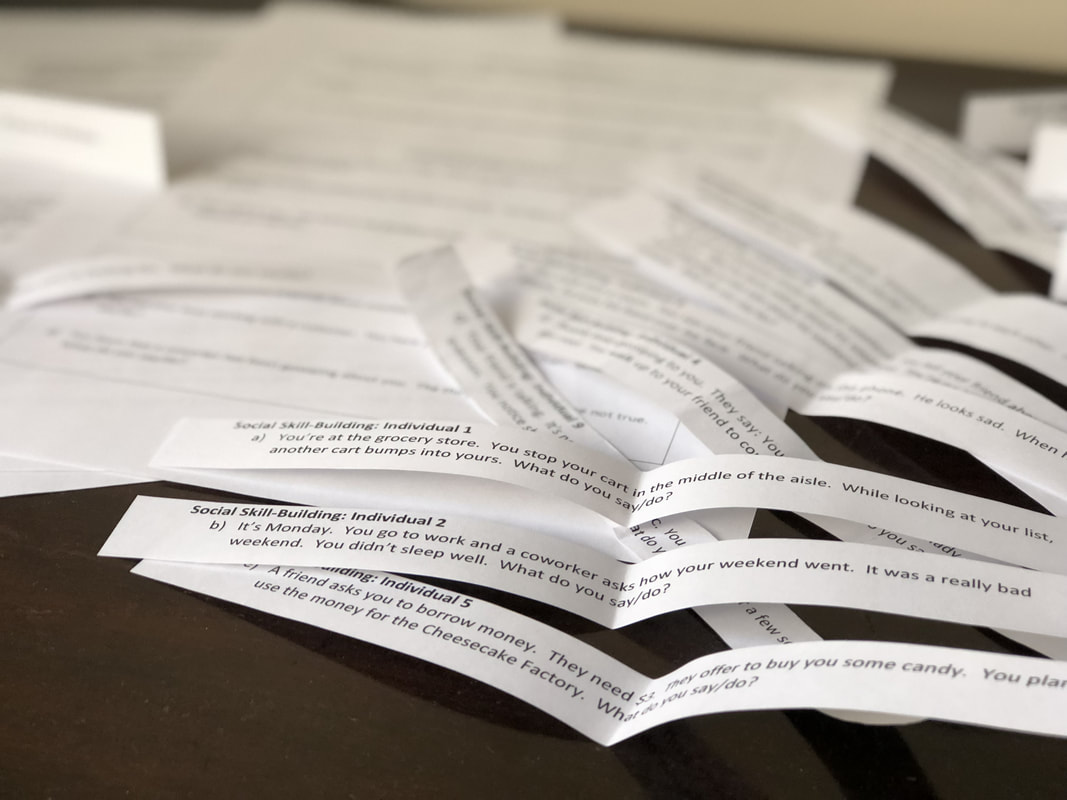
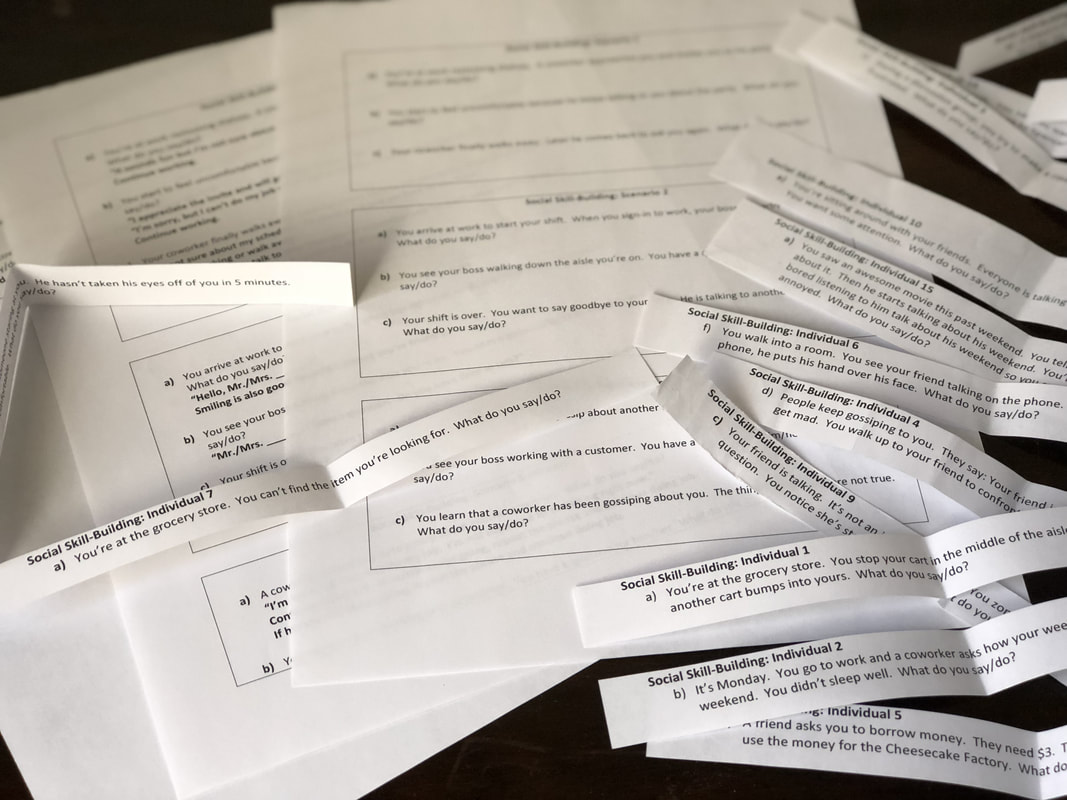
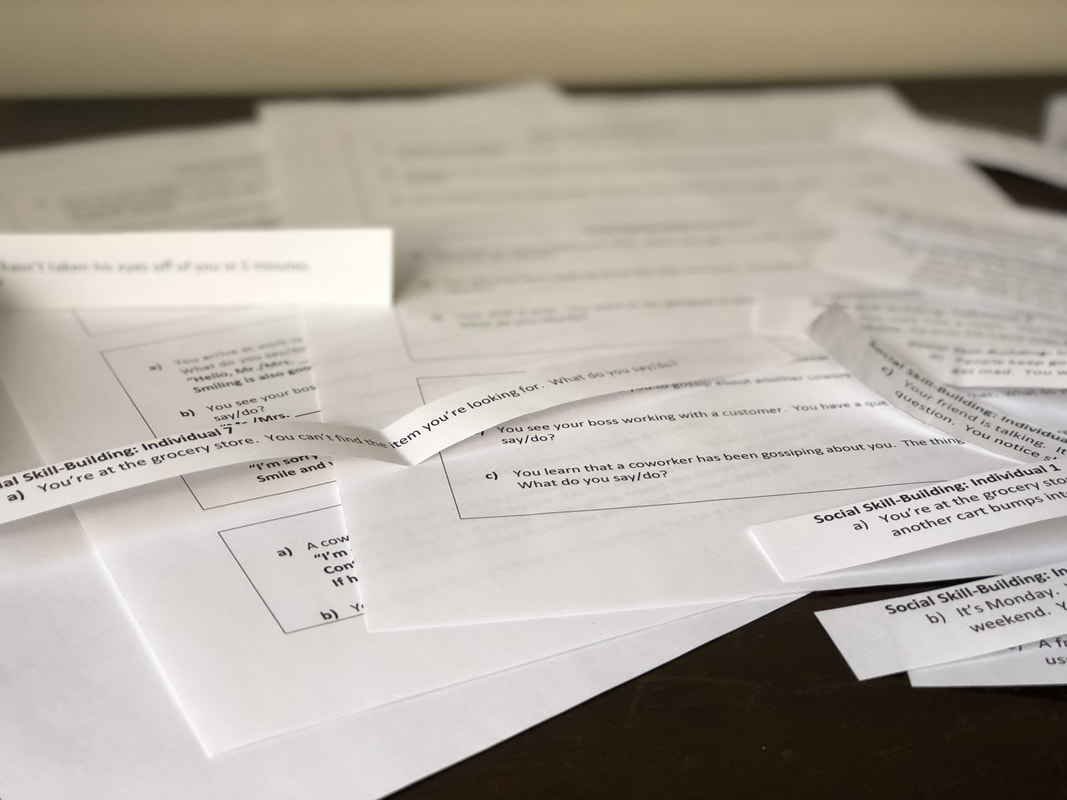
Based on this experience, I can see why it's important to advocate for my clients. There's a saying that "OTs only see their clients for an hour of the day, once a day or a week, but their families see them every day for multiple hours on end." Carryover is an important part of the process. This means that whatever is practiced in therapy should also be practiced at home in order for the individual to recognize that the skills learned in one setting can be applied in other settings. I had the opportunity to advocate for my client one more time by providing the other staff members with materials to continue working on with the client. The ones who were interested though, I heavily encouraged to carryover those skills with her because she would continue to grow and learn, even after my time at this fieldwork site ended.
Based on her interview, I was able to gather that my client did not receive as much help in developing basic social skills needed to successfully transition into the community post-graduation. This may have been due to cultural and environmental influences. Nevertheless the stigma of her intellectual disability limited her ability to participate in certain activities at home, at school, and in the community. She was continuously restricted to certain tasks over her lifetime she felt incompetent to try something new. For instance, she would stick to tasks she knew how to do because she had always done it at home or school. The same held true for new social experiences: she was uncomfortable interacting with anyone outside of her family. This resulted in her lack of desire to try new things and led her to believe she would never be able to live without a caregiver. Due to this lack of experience, it may have resulted in poor social skills. I learned that individuals with schizoaffective disorder not only have difficulty expressing themselves through facial expressions, tone, and body language, but they also have difficulty reading these nonverbal cues in others. Her dual diagnosis may have made it even more difficult to appropriately interact with others and led to social problems while in the community. This was one of the major reasons for my client to attend this program because she needed to improve her social interaction skills.
Towards the end of this interview, I learned that this young lady was a motivated individual who wanted to improve her social skills in order to eventually hold a job for more than a few months. Regardless of her intellectual disability and her mental illness, her motivation would be the catalyst to her overall success when working toward her social skills goal. Although I have worked with individuals with intellectual disabilities since high school, and I have seen numerous times that they are capable of learning something new, even at a slower pace, I had never worked with an individual with a dual diagnosis like this. The same was true for some of my other coworkers who had acknowledged to me that they were less familiar with individuals with intellectual disabilities, and more so with a dual diagnosis. I considered this to be an educational opportunity for both me and my coworker, but I also considered this to be a chance for me to advocate for this particular individual.
I started advocating for this individual to other staff members at my facility.
Luckily, they understood what I was saying, and gave me free reign to work with her. She was motivated to get started. Although she required frequent one-on-one sessions and repetition, her efforts began to show as she started making progress in her goals.
Based on this experience, I can see why it's important to advocate for my clients. There's a saying that "OTs only see their clients for an hour of the day, once a day or a week, but their families see them every day for multiple hours on end." Carryover is an important part of the process. This means that whatever is practiced in therapy should also be practiced at home in order for the individual to recognize that the skills learned in one setting can be applied in other settings. I had the opportunity to advocate for my client one more time by providing the other staff members with materials to continue working on with the client. The ones who were interested though, I heavily encouraged to carryover those skills with her because she would continue to grow and learn, even after my time at this fieldwork site ended.
